 Coincidence scan of a canine, courtesy of: http://ecpi.crump.ucla.edu/vol2/issue4/matwichuk/matwichuk_case-ex.html
Coincidence scan of a canine, courtesy of: http://ecpi.crump.ucla.edu/vol2/issue4/matwichuk/matwichuk_case-ex.html
Actually, there are numerous options out there for those in the market to purchase a PET scanner. I've directed the purchase of three over the years. My first "PET" scanner was a coincidence device from ADAC, which was replaced with a Siemens ECAT Exact 47, and then with a Siemens Biograph 16 Hybrid PET/CT. As I mentioned in a prior post, GE lobbied me heavily to buy a Discovery ST instead, but I was convinced that the faster LSO crystals in the Biograph made it the best choice.
Fast-forward to the present. My group has today a rather unique situation: we read PET/CT studies from the Siemens I chose, and from a Discovery ST placed several months later at the oncology clinic we cover. So, we can do some near-direct comparisons. I say "near-direct" because we don't have the workstations for the competing systems side by side, and even when a patient has a prior exam, comparisons are done with a CD-ROM or on PACS, which is not the optimal way to do this. (I should, of course, add that about 99% of the time, the new scan is at the clinic and the old was from the hospital, which shouldn't surprise anyone.)
I'll give you the punchline first, and then we'll go into the boring discussion of what's behind it. My educated, although still subjective, opinion is that the Biograph produces better images. Sorry, GE, but Siemens gives us images with less noise which are overall more pleasing and easier to read, again, in my opinion. The faint of heart can leave now.
A word about the proprietary workstations attached to each camera is in order. GE provides the Advantage Workstaton 4.3, the AW, and Siemens uses the Leonardo with eSoft. To be fair, I find the Linux-based AW about the same in ease of use for this application, although it helps that the apps people set me up with my own hanging-protocol. The Windows-based Leo got a slightly different version of my custom display. I don't really like the AW for other purposes, but for PET/CT it works well enough. There are numerous differences in the overall approaches, and I tend to prefer the Leo for CT. Both lack mouse-wheel scrolling, which would be a welcome addition.
The two scanners themselves are quite different in their hearts, their detector crystals, and their approach to the actual acquision of the image.
For those unfamiliar with positron scanning, a very brief primer is in order. Positrons are positively-charged particles that are otherwise identical to negatively-charged electrons. The positron is technically antimatter, which does exist outside of the Star Trek universe. Isotopes that emit positrons when they decay are made by cyclotron, and the most common is 18F, or Flourine-18, which has a half-life of 110 minutes. (Half-life means that half of the stuff is gone or transformed, within that time.) For PET scanning, we label a glucose analogue with 18F to get 18-FDG, fluorodeoxyglucose. This can be used to map metabolism, taking advantage of the fact that most tumors and other bad things burn glucose faster than most normal tissues.
When the 18F decays, it shoots off its positron, which quickly comes in contact with one of the vastly more numerous electrons in the adjacent tissues (or air, or whatever). When a positron meets an electron, they annihilate each other, with a very tiny "bang," and in the process sends out two photons, each with the energy of 511 KeV (Kiloelectron Volts) which just happens to be the amount of energy contained in the mass of the electron or the positron. As it turns out, it is these photons, which are sent out at 180 degrees opposed to each other, which are detected, and not the positrons per se. Thus, we really should call this whole process "Annihilation Imaging" and not PET scanning, but I doubt that anyone would stick their head in an "Annihilation Scanner"!

Siemens uses Lutetium Oxyorthosilicate, or LSO, crystals, pictured below, while GE uses Bismuth Germinate (which looks quite similar.)

OK, a crystal is a crystal, right? Well, not really. The purpose of the crystal is to turn those 511 KeV photons into light, which is then turned into an electrical signal, and then into the picture. To make a long story short, LSO does a better job of turning the radiation into light, and does it more quickly than BGO, so it can handle a higher amount of radiation. Now, GE insisted that BGO is just as good, and sent me a barrage of articles to prove this. However, GE is working on its own version of LSO, called LYSO, and rumor has it that Duke, the main showsite for GE PET, will not get another PET/CT scanner until GE can deliver the LYSO unit. (The GE people tell me that they are making LYSO to accomodate future PET pharmaceuticals, and BGO is really great for now.)
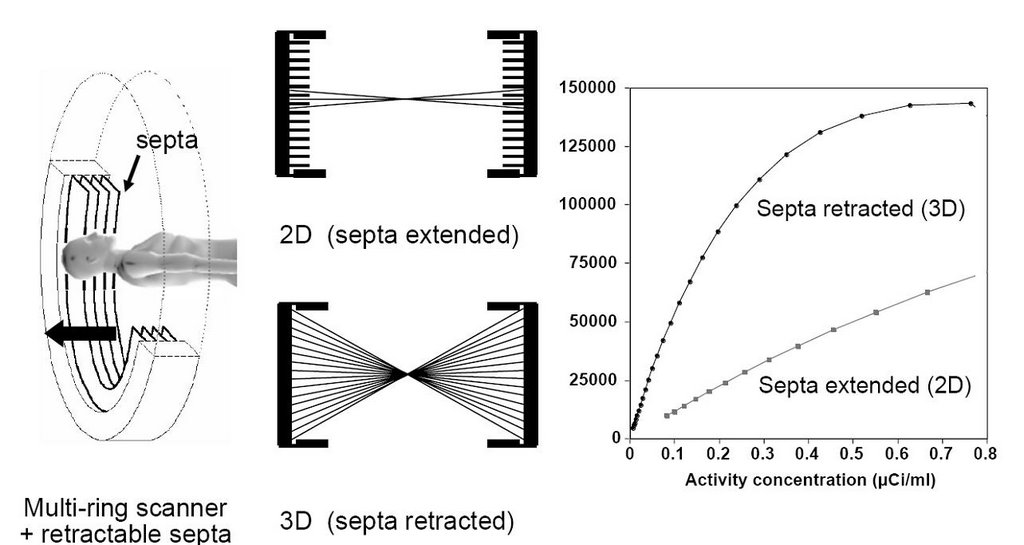
But there's even more to the story. The PET portion of a PET/CT gantry isn't just a big tube-shaped crystal, but rather a collection of smaller crystals arranged in rings. When a detector senses an annihilation photon, it tries to match it to another one that came in at the same time. The simultaneity allows the machine to figure out where the detonation occurred and then it can paint the picture of the distribution of the tracer. But sometimes the radiation gets scattered within the body, or two unconnected (random) photons happen to hit at the same time. To prevent this, thick lead septa are introduced as in the image below..this is the so-called 2-dimensional approach. With faster crystals, it is theoretically easier to discriminate on the time of arrival, and so one can open up the whole array of detectors to receive all possible photons, the so-called 3-dimensional approach. Siemens LSO PET/CT's use 3D exclusively, while GE's BGO machines can run in either 3D or 2D mode.
“From 3D PET to 3D PET/CT: what did we learn?” Peter Valk Lecture given by David W. Townsend, Ph.D.,
Department of Medicine and Radiology University of Tennessee, Knoxville
All well and good. Again, to make a long story very short, the 3D approach allows a lot more scatter radiation and random counts to be, well, counted. On the other hand, 3D picks up a whole lot more photons overall. Do these balance out? The answer depends on the article you read. Here is one from a recent article in the Journal of Nuclear Medicine by Lodge, et. al.:
Italics are mine, as usual. Now GE cited some other articles contradicting this one. One in particular by Laritizien, et. al., states:
Comparisons of 2D and 3D performance are very sensitive to the specific conditions under which the data were acquired. Counting rate, scatter, activity outside the field of view, reconstruction algorithm, and scanner characteristics all influence relative performance. In this study 2D and 3D data were compared under clinically realistic conditions and effects that may introduce bias were minimized. The mean ratio of 3D to 2D image values was 0.94 with 95% limits of agreement of 0.63–1.41. All noise comparisons were made under conditions of matched lesion target-to-background ratio as measured in patient images. A statistically significant reduction in image noise was found with 3D acquisition compared with 2D, suggesting reductions in scan duration of 33% or more are feasible.
In this study, we performed an AFROC analysis to evaluate the impact of the acquisition mode (2D vs. fully 3D) on human observer detection performances. Three acquisition protocols were selected to provide a fair comparison between the acquisition modes. Results showed that the fully 3D acquisition mode allowed better or equivalent detection performance than the 2D mode for a same injected dose typical of the clinical practice (about 440 MBq) in a standard patient. The 2D acquisition protocol combined with higher injected doses (about 740 MBq) resulted in higher detectability than those achieved with the fully 3D acquisition mode for approximately half the injected dose. Changing the patient size or the PET scanner model will potentially change the lesion detectability results of this study.
Now, wait just a second. This says you have to double the dose to get 2D to work better in the clinical setting than 3D! That's problematic enough, but, BGO has a slower response than LSO, and the "dead time", the time it takes the crystal to "recover" from the last event could get to be a problem if you really crank up the dose. I won't even go into the wisdom of doubling the radiation dose, although 18F is short-lived. Basically, we are not comparing apples and apples here.
One way to improve your pictures with either system is to scan longer. We had a 2D BGO system, as you may recall, the Siemens ECAT Exact 47, and we scanned at 7-minutes per bed position, i.e., how long each segment of the patient is within the ring of detectors. GE has advised its Discovery ST customers that 2-3 minutes is plenty adequate. Now, I'll grant you that some significant electronics improvements have occured between the introductions of the two devices, but have there been enough to drop scan time by more than half (not counting the time for the attenuation scan, either with the old germanium transmission or with the faster CT version)? I don't know. What I do know is that the images from the Biograph are better, at least to me, than those from the Discovery. That's my story, and I'm sticking to it.
GE made a last ditch effort to change our minds by reminding us that they won the Frost & Sullivan Market Leadership Award for the PET/CT in 2004. This is a monumental achievement, true, but take a look at the press release from Frost & Sullivan:
Frost & Sullivan’s recent analysis, U.S. PET and PET-CT Markets, selected GE Healthcare as the recipient of the 2004 Market Leadership Award. This Award acknowledges the company’s exceptional marketing strategies that helped it capture the largest percentage of the U.S. positron emission tomography-computed tomography (PET-CT) market in 2003 and maintain its robust lead since the market’s inception.I have to agree 100%. GE certainly has exceptional marketing strategy. No question about that. But I don't think Frost & Sullivan is really qualified to evaluate the scanners themselves. That needs to be left to those of us who actually have to interpret the images. You might ask, "Will the Discovery fail to demonstrate something that the Biograph would show?" Now that's one question I can't honestly answer, and it's probably the most important of all. Time will tell on that one. But you can bet it will become obvious eventually.
No comments :
Post a Comment