There aren't too many pictures that come up when you search for "RIS", so how about a flourless chocolate cake instead? RIS-less, flourless, what's the difference?
This post may disturb my friend Mark, who recently left Amicas for Empiric Systems, the creators of a very nice web-based Radiology Information System, or RIS. I am going to tell you how I'm going to forgo purchasing his product for my independent PACS operation, and that means he won't be selling me one for a while. It's a great system, but I need to trim my costs where possible.
Speaking of Marks...some of you may know I tried to hire back a PACS guru named Mark M., who was driven out of town for various reasons by a certain IT empire. Fortunately for him, but unfortunately for me, he likes his new spot, and he couldn't be lured back to my place. But Fate always has something interesting up her sleeve. Our PA came to me one day and said, "I know this really great PACS guy, who might be interesting in your weird, I mean progressive ideas. He is thinking about moving, so why don't we get in touch with him?" What's his name? Mark S! Must be karma again. He came to look around, liked what he saw, and we now have our PACS guru. He is already hard at work creating our independent system, and I'll report back as we progress.
Anyway, back to RIS's or the lack thereof. To achieve the RIS-less RIS, you must first define what you need out of such a contraption. At the bare minimum, we need to attach demographics and reports to a study. Yes, a RIS can provide much more than that, but keep in mind, the clients for our little operation are mainly clinicians with scanners in their offices (DON'T even say it...), with relatively small volumes and internal billing and scheduling. Therefore, we can stick to the very basics, at least for now.
I have mentioned PACSGEAR in earlier posts, and I had the chance to meet some of their staff and play with their products at RSNA. They offer two products that solve my "RISsy"-fit, and later I'll tell you about a third that is really nice.

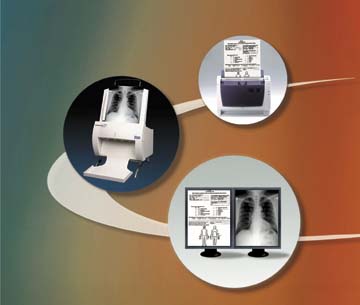
This illustrates the concept: You have a sheet of demographics, history, or whatever that you want the rad to have available with the scan. With the PACSGEAR PacsSCAN program, you just scan the piece of paper with a regular old TWAIN document scanner (they recommend a heavy-duty version rather than the $25 Best-Buy bargain), bring up 

the patient in question via the little dialogue window ("Lookup" will fetch the pertinent info from your PACS or RIS if you have one), and off you go. Just press SCAN and the document becomes yet another DICOM sequence in the designated exam. Couldn't be easier.
Print2PACS does something similar, but instead of scanning a physical document, you quite literally print a DICOM image into your examination. With this little program, our transcriptionists can print the report straight into the system, where it can be viewed along with the rest of the examination. Print2PACS makes it possible to store other things like DEXA or cath reports, or even JPEG images if you have a need to do so. Now, this isn't a perfect solution. What you get on the viewing end is a picture of a report, and it can't be edited or minipulated. (I suppose you could play with its window and level, and magnify it if you wanted, but you can't change any of the words.) Still, it gets the report in front of the clinician, which is the goal.
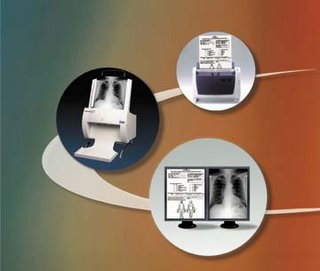 The third product in the PACSGEAR suite is one that doesn't really contribute to the RIS idea, but it is great for our purposes none the less. PacsSCAN Film adds a film digitizer to the picture, if you will, and will scan yucchy old film into your shiny new PACS system. But it goes one step beyond just digitizing...it will divide out sheets of multiple images into understandable sequences that fit right in on the PACS workstation. No more big picture full of smaller images that you have to pan around to view. This is a great thing for those of us reading from sites who are still filming.
The third product in the PACSGEAR suite is one that doesn't really contribute to the RIS idea, but it is great for our purposes none the less. PacsSCAN Film adds a film digitizer to the picture, if you will, and will scan yucchy old film into your shiny new PACS system. But it goes one step beyond just digitizing...it will divide out sheets of multiple images into understandable sequences that fit right in on the PACS workstation. No more big picture full of smaller images that you have to pan around to view. This is a great thing for those of us reading from sites who are still filming.
I have to add that there are free programs out there that do much of what we're talking about here, basically converting .TIFF or conventional print files to DICOM. I've played with some of them, and while they do actually work rather well (especially for being free), they are not as smooth and elegant as the PACSGEAR products. Therefore, PACSGEAR gets the Dalai Seal of Usability. I'm looking forward to being one of their customers.